
DUPIXENT® in chronic obstructive pulmonary disease (COPD) with an eosinophilic phenotype
Patients aged 18+ years
DUPIXENT IS THE FIRST AND
ONLY BIOLOGIC APPROVED IN
COPD1
Limitations of Use: DUPIXENT is not indicated for the relief of acute
bronchospasm.
DUPIXENT WAS STUDIED ACROSS 2 CLINICAL TRIALS, BOREAS AND NOTUS

Adults aged
40+ years
BOREAS and NOTUS clinical study designs1,a
Two Phase 3 trials evaluated the efficacy of DUPIXENT + standard of careb administered every 2 weeks in patients with inadequately controlled COPD.1,b
Standard of care was triple inhaled therapy (LAMA + LABA + ICS.2
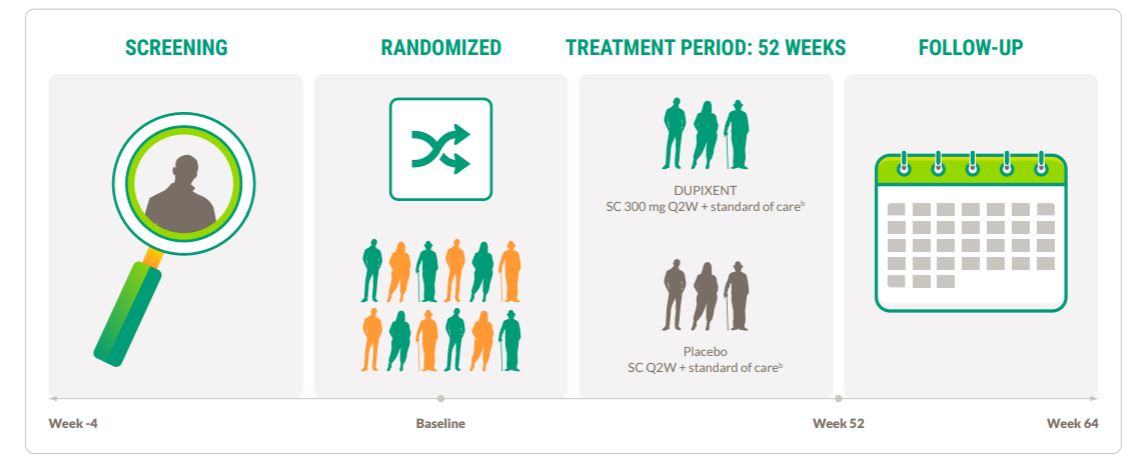
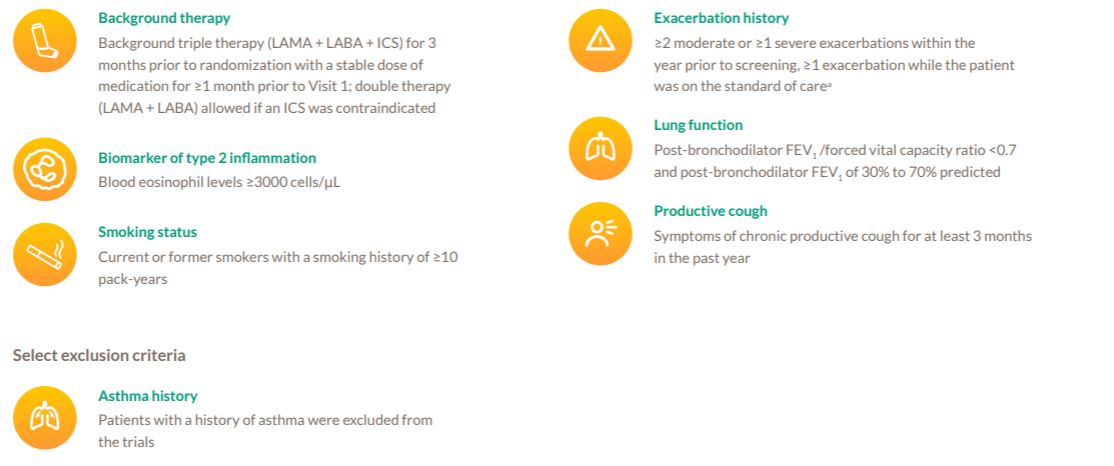
Patients with a history of asthma were excluded from the BOREAS and NOTUS trials.
a1874 patients were enrolled in the BOREAS (N=939) and NOTUS (N=935) trials.1
b98% received LAMA + LABA + ICS in BOREAS and 99% in NOTUS.1
COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; Q2W, once every 2 weeks; SC, subcutaneous.
Study designs: endpoints1
| PRIMARY ENDPOINT | Week 52 | Annualized rate of moderate or severe COPD exacerbations |
|---|---|---|
| SELECT SECONDARY ENDPOINTS | Week 12
Week 52 |
Change in lung function (pre-bronchodilator FEV₁) from baseline |
| Week 52 | Change in SGRQ total score from baseline | |
| Week 52 | Percentage of patients with SGRQ total score improvement of ≥4 points |
FEV1, forced expiratory volume in 1 second; SGRQ, St. George’s Respiratory Questionnaire.
Study designs: inclusion and exclusion criteria3,4
aModerate exacerbations were defined as exacerbations that resulted in treatment with a systemic glucocorticoid, an antibiotic agent, or both. Severe exacerbations were defined as exacerbations that led to hospitalization or an emergency medical care visit or that resulted in death.1
DUPIXENT was studied in key disease outcomes that reflect the debilitating nature of COPD1
aModerate exacerbations were defined as exacerbations that resulted in treatment with a systemic glucocorticoid, an antibiotic agent, or both.1
bSevere exacerbations were defined as exacerbations that led to hospitalizations or an emergency medical care visit or that resulted in death.1
cSGRQ total score is a patient self-measure of cough, sputum production, breathlessness, and wheezing, as well as disturbances to daily physical activity and psychosocial function. The SGRQ is a 50-item questionnaire designed to measure and quantify health status in adult patients with chronic airflow limitation. Higher score indicates greater disease severity.5
FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroid; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; SGRQ, St. George’s Respiratory Questionnaire.
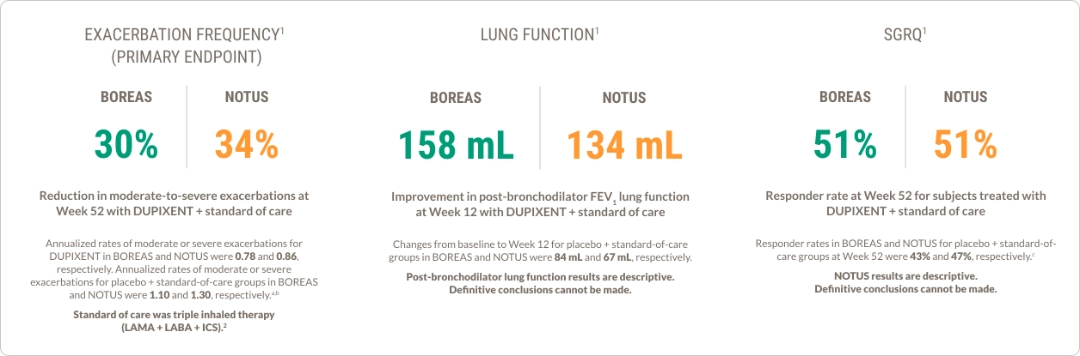
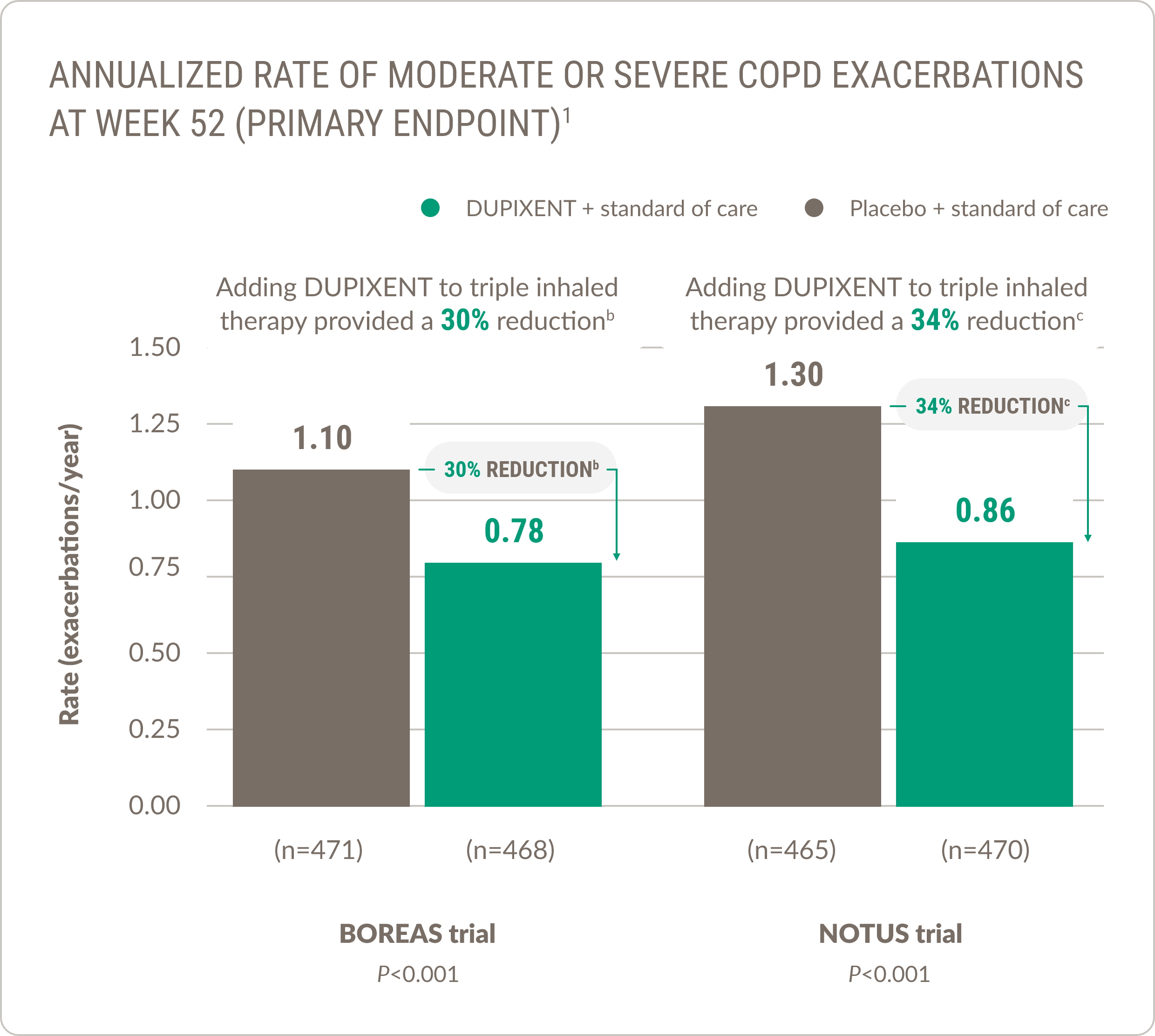
DUPIXENT significantly reduced COPD exacerbations1,a
When added to the standard of care, DUPIXENT significantly reduced the annualized rate of moderate or severe exacerbations1

Exacerbations are associated with increased costs6
Standard of care was triple inhaled therapy: LAMA + LABA + ICS.2
aModerate exacerbations were defined as exacerbations that resulted in treatment with a systemic glucocorticoid, an antibiotic agent, or both. Severe exacerbations were defined as exacerbations that led to hospitalization or an emergency medical care visit or that resulted in death.1
bRate ratio vs placebo: 0.71 (95% CI: 0.58, 0.86).1
cRate ratio vs placebo: 0.66 (95% CI: 0.54, 0.82).1
DUPIXENT showed improvement in lung function1
Lung function improvement sustained through Week 521
|
Post-bronchodilator FEV1 BOREAS trial1 |
Post-bronchodilator FEV1 NOTUS trial1 |
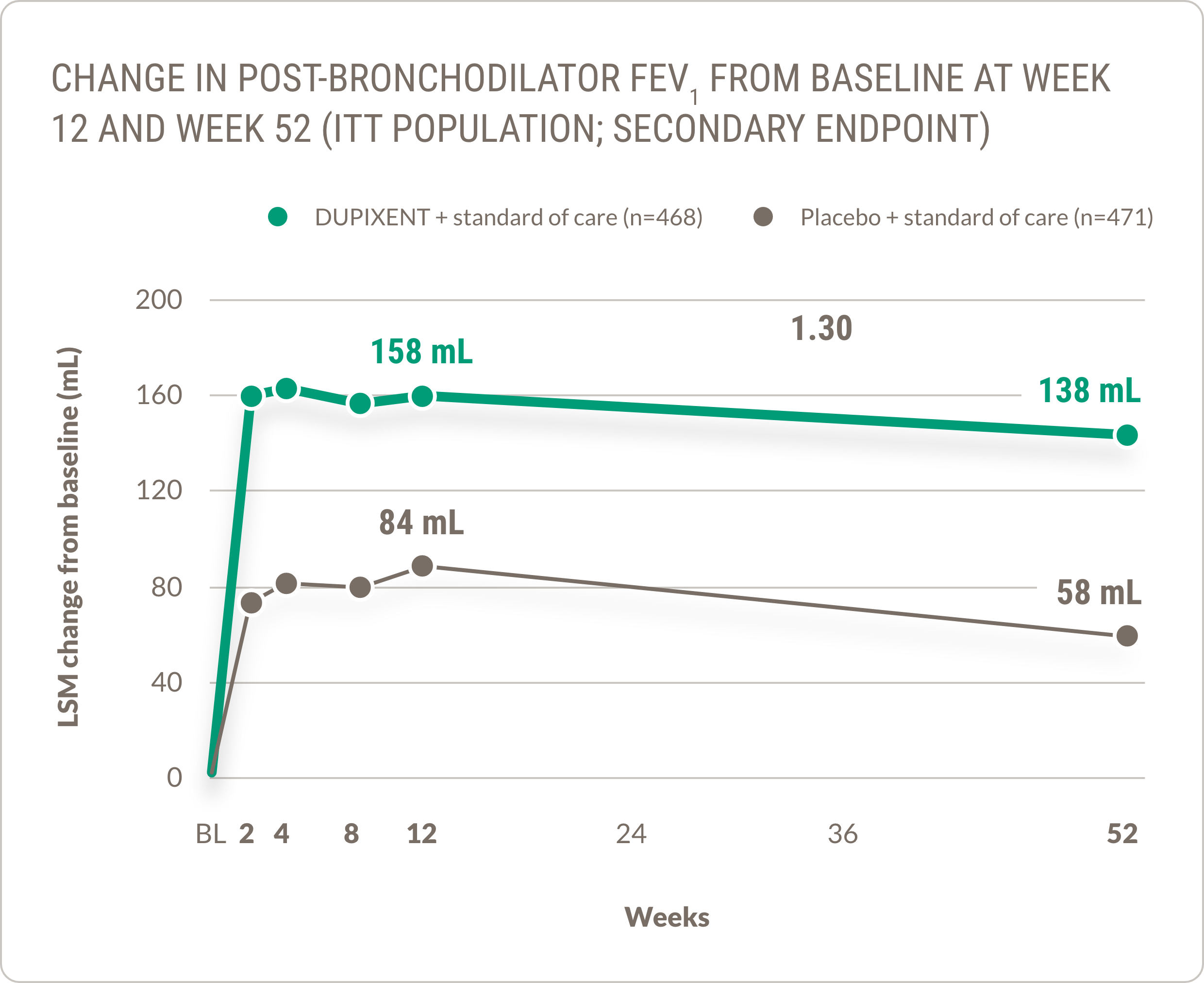
Patients administered DUPIXENT + standard of care saw numerical improvement in post-bronchodilator FEV1 of 134 mL at Week 12 (n=470) and 127 mL at Week 52 (n=362), compared with 67 mL at Week 12 (n=465) and 59 mL at Week 52 (n=359) in patients receiving placebo + standard of care (LSM change from baseline, ITT population).
Lung function impairment and disease severity are associated with increased costs7
Pre-bronchodilator FEV1
Significant improvements of similar magnitude were observed in change from baseline in pre-bronchodilator FEV1 at Weeks 12 and 52 in subjects treated with DUPIXENT compared with placebo across the BOREAS and NOTUS trials.1
Post-bronchodilator lung function results are descriptive. Definitive conclusions cannot be made.
Standard of care was triple inhaled therapy (LAMA + LABA + ICS).2
BL, baseline; ITT, intent to treat; LSM, least squares mean.
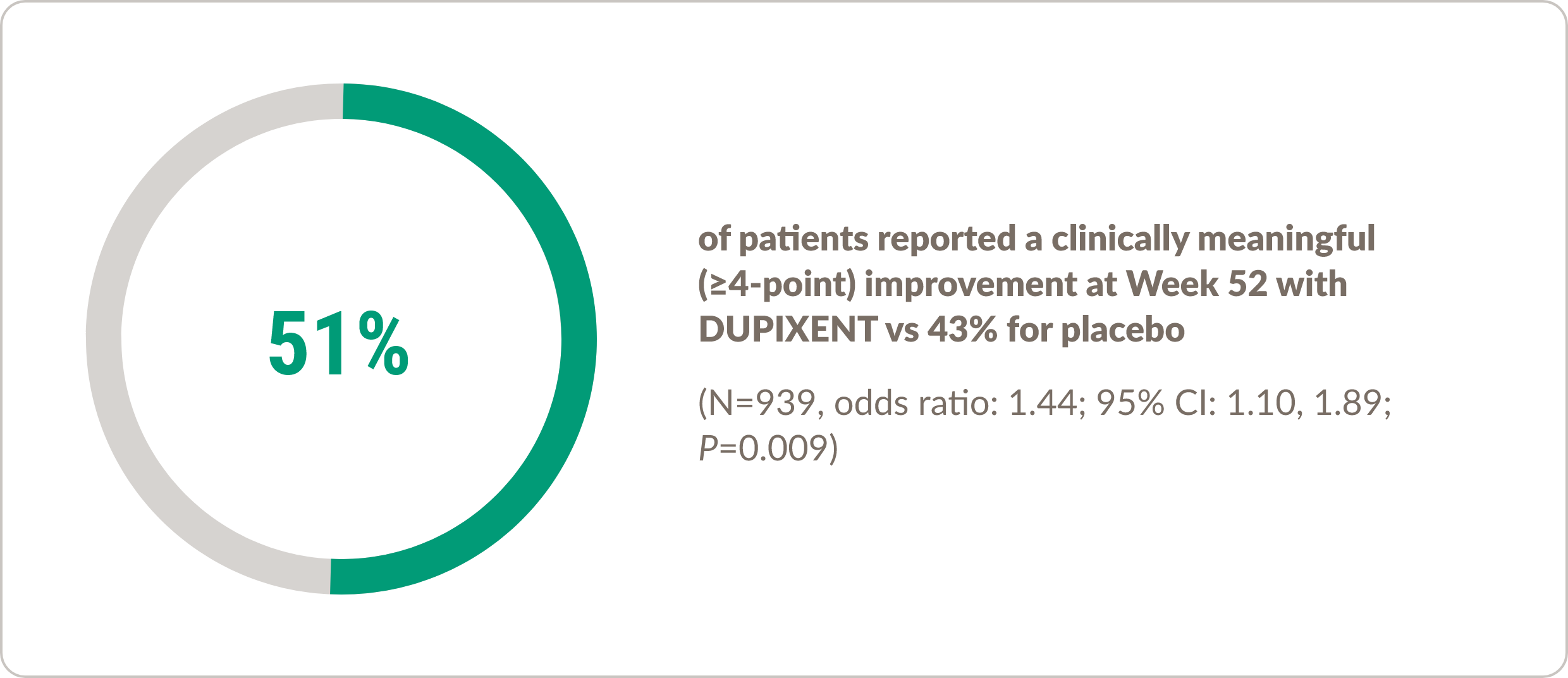
DUPIXENT improved COPD patients’ daily quality of life as measured by SGRQ1,a
BOREAS trial1

Standard of care was triple inhaled therapy (LAMA + LABA + ICS).2
NOTUS trial1
There was a 51% responder rate at Week 52 for subjects treated with DUPIXENT vs 47% for placebo (N=721, odds ratio: 1.16; 95% CI: 0.86, 1.58).
NOTUS results are descriptive. Definitive conclusions cannot be made.
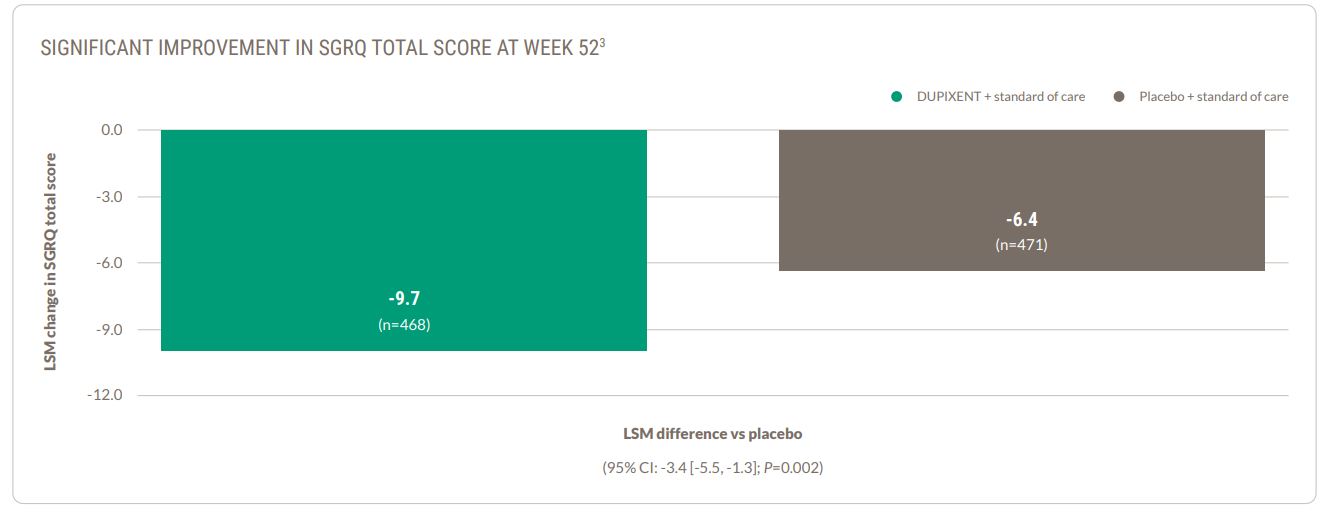
DUPIXENT improved SGRQ total score at Week 52 1
DUPIXENT improved SGRQ total score at Week 521
DUPIXENT reduced SGRQ scores—lower SGRQ scores indicate improved quality of life.1,3,4
BOREAS trial 3
BOREAS trial 3
In NOTUS, patients receiving DUPIXENT + standard of care (n=362) experienced -9.8 reduction in total SGRQ score vs -6.4 in patients with placebo + standard of care (n=359) (LSM difference: -3.4 [95% CI: -5.8, -0.9])
NOTUS results are descriptive. Definitive conclusions cannot be made.
Standard of care was triple inhaled therapy (LAMA + LABA + ICS.2
ICS, inhaled corticosteroid; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; LSM, least squares mean; SGRQ, St. George’s Respiratory Questionnaire
Worsening quality of life may lead to higher costs8
aSGRQ is a disease-specific instrument designed to measure impact on overall health, daily life, and perceived well-being in patients with COPD.
Demonstrated safety profile in COPD through 52 weeks1
| ADVERSE REACTION | BOREAS and NOTUS | |
|---|---|---|
| DUPIXENT 300 mg Q2W
N=938 n (%) |
Placebo
N=934 n (%) |
|
| Viral infectiona | 133 (14.2) | 115 (12.3) |
| Headache | 73 (7.8) | 62 (6.6) |
| Nasopharyngitis | 73 (7.8) | 69 (7.4) |
| Back pain | 42 (4.5) | 29 (3.1) |
| Diarrheaa | 35 (3.7) | 30 (3.2) |
| Arthralgia | 29 (3.1) | 25 (2.7) |
| Urinary tract infection | 28 (3.0) | 18 (1.9) |
| Local administration reactions
Injection site reactions |
26 (2.8)
11 (1.2) |
6 (0.6)
2 (0.2) |
| Rhinitis | 24 (2.6) | 17 (1.8) |
| Eosinophiliab | 22 (2.3) | 7 (0.7) |
| Toothache | 20 (2.1) | 11 (1.2) |
| Gastritis | 19 (2.0) | 7 (0.7) |
aConsists of multiple similar terms.
bEosinophilia was defined as blood eosinophils ≥3000 cells/μL or deemed by the investigator to be an adverse event. None met the criteria for serious eosinophilic conditions.
Q2W, once every 2 weeks.

The DUPIXENT value for your plan
Explore the value of the only biologic treatment approved in 8 indications driven in part by type 2 inflammation.
-
Explore the other indications of DUPIXENT
Moderate-to-severe eosinophilic or
OCS-dependent asthma
(aged 6+ years)
Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm or status asthmaticus.
Inadequately controlled chronic rhinosinusitis with nasal polyps (aged 12+ years)
Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm.
Symptomatic chronic spontaneous urticaria despite H1 antihistamine treatment (aged 12+ years)
Limitations of Use: DUPIXENT is not indicated for treatment of other forms of urticaria.
References: 1. DUPIXENT. Prescribing information. Regeneron Pharmaceuticals, Inc.; 2024. 2. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2024 report. Accessed May 8, 2024. https://goldcopd.org/2024-gold-report/ 3. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with type 2 inflammation indicated by eosinophil counts. N Engl J Med. 2023;389(3):205-214. doi:10.1056/NEJMoa2303951 4. Bhatt SP, Rabe KF, Hanania NA, et al. Dupilumab for COPD with blood eosinophil evidence of type 2 inflammation. N Engl J Med. 2024;390(24):2274-2283. doi:10.1056/NEJMoa2401304 5. Jones PW, Forde Y. St. George’s Respiratory Questionnaire Manual. Version 2.4. St. George’s University of London; 2022. 6. Blanchette CM, Gross NJ, Altman P. Rising costs of COPD and the potential for maintenance therapy to slow the trend. Am Health Drug Benefits. 2014;7(2):98-106. 7. Wallace AE, Kaila S, Bayer V, et al. Health care resource utilization and exacerbation rates in patients with COPD stratified by disease severity in a commercially insured population. J Manag Care Spec Pharm. 2019;25(2):205-217. doi:10.18553/jmcp.2019.25.2.205 8. Ridolo E, Pellicelli I, Gritti B, Incorvaia C. Patient-reported outcomes and considerations in the management of COPD: focus on indacaterol/glycopyrronium bromide. Patient Prefer Adherence. 2019;13:145-150. doi:10.2147/PPA.S166704
INDICATIONS
Atopic Dermatitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 6 months and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. DUPIXENT can be used with or without topical corticosteroids.
Asthma: DUPIXENT is indicated as an add-on maintenance treatment of adult and pediatric patients aged 6 years and older with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm or status asthmaticus.
Chronic Rhinosinusitis with Nasal Polyps: DUPIXENT is indicated as an add-on maintenance treatment in adult and pediatric patients aged 12 years and older with inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP).
Eosinophilic Esophagitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 1 year and older, weighing at least 15 kg, with eosinophilic esophagitis (EoE).
Prurigo Nodularis: DUPIXENT is indicated for the treatment of adult patients with prurigo nodularis (PN).
Chronic Obstructive Pulmonary Disease: DUPIXENT is indicated as an add-on maintenance treatment of adult patients with inadequately controlled chronic obstructive pulmonary disease (COPD) and an eosinophilic phenotype. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm.
Chronic Spontaneous Urticaria: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 12 years and older with chronic spontaneous urticaria (CSU) who remain symptomatic despite H1 antihistamine treatment. Limitations of Use: DUPIXENT is not indicated for treatment of other forms of urticaria.
Bullous Pemphigoid: DUPIXENT is indicated for the treatment of adult patients with bullous pemphigoid (BP).
CONTRAINDICATION: DUPIXENT is contraindicated in patients with known hypersensitivity to dupilumab or any of its excipients.
WARNINGS AND PRECAUTIONS
Hypersensitivity: Hypersensitivity reactions, including anaphylaxis, acute generalized exanthematous pustulosis (AGEP), serum sickness or serum sickness-like reactions, angioedema, generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. A case of AGEP was reported in an adult subject who participated in the bullous pemphigoid development program. If a clinically significant hypersensitivity reaction occurs, institute appropriate therapy and discontinue DUPIXENT.
Conjunctivitis and Keratitis: Conjunctivitis and keratitis occurred more frequently in AD, COPD, and BP subjects who received DUPIXENT versus placebo, with conjunctivitis being the most frequently reported eye disorder in AD. Conjunctivitis also occurred more frequently in adult CRSwNP and PN subjects who received DUPIXENT compared to those who received placebo. Conjunctivitis and keratitis have been reported with DUPIXENT in postmarketing settings, predominantly in AD patients. Some patients reported visual disturbances (e.g., blurred vision) associated with conjunctivitis or keratitis. Advise patients or their caregivers to report new-onset or worsening eye symptoms. Consider ophthalmological examination for patients who develop conjunctivitis that does not resolve following standard treatment or signs and symptoms suggestive of keratitis, as appropriate.
Eosinophilic Conditions: Patients being treated for asthma may present with clinical features of eosinophilic pneumonia or eosinophilic granulomatosis with polyangiitis (EGPA). These events may be associated with the reduction of oral corticosteroid therapy. Healthcare providers should be alert to vasculitic rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and/or neuropathy presenting in their patients with eosinophilia. Cases of eosinophilic pneumonia were reported in adults who participated in the asthma development program and cases of EGPA have been reported with DUPIXENT in adults who participated in the asthma development program as well as in adults with co-morbid asthma in the CRSwNP development program. Advise patients to report signs of eosinophilic pneumonia and EGPA. Consider withholding DUPIXENT if eosinophilic pneumonia or EGPA are suspected.
Acute Symptoms of Asthma or Chronic Obstructive Pulmonary Disease or Acute Deteriorating Disease: Do not use DUPIXENT to treat acute symptoms or acute exacerbations of asthma or COPD, acute bronchospasm, or status asthmaticus. Patients should seek medical advice if their asthma or COPD remains uncontrolled or worsens after initiation of DUPIXENT.
Risk Associated with Abrupt Reduction of Corticosteroid Dosage: Do not discontinue systemic, topical, or inhaled corticosteroids abruptly upon initiation of DUPIXENT. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a healthcare provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
Patients with Co-morbid Asthma: Advise patients with co-morbid asthma not to adjust or stop their asthma treatments without consultation with their physicians.
Psoriasis: Cases of new-onset psoriasis have been reported with the use of DUPIXENT for the treatment of atopic dermatitis and asthma, including in patients without a family history of psoriasis. In postmarketing reports, these cases resulted in partial or complete resolution of psoriasis with discontinuation of dupilumab, with or without use of supplemental treatment for psoriasis (topical or systemic). Those who continued dupilumab received supplemental treatment for psoriasis to improve associated symptoms. Advise patients to report new-onset psoriasis symptoms. If symptoms persist or worsen, consider dermatologic evaluation and/or discontinuation of DUPIXENT.
Arthralgia and Psoriatic Arthritis: Arthralgia has been reported with the use of DUPIXENT with some patients reporting gait disturbances or decreased mobility associated with joint symptoms; some cases resulted in hospitalization. Cases of new-onset psoriatic arthritis requiring systemic treatment have been reported with the use of DUPIXENT. Advise patients to report new-onset or worsening joint symptoms. If symptoms persist or worsen, consider rheumatological evaluation and/or discontinuation of DUPIXENT.
Parasitic (Helminth) Infections: It is unknown if DUPIXENT will influence the immune response against helminth infections. Treat patients with pre-existing helminth infections before initiating therapy with DUPIXENT. If patients become infected while receiving treatment with DUPIXENT and do not respond to anti-helminth treatment, discontinue treatment with DUPIXENT until the infection resolves. Helminth infections (5 cases of enterobiasis and 1 case of ascariasis) were reported in pediatric patients 6 to 11 years old in the pediatric asthma development program.
Vaccinations: Consider completing all age-appropriate vaccinations as recommended by current immunization guidelines prior to initiating DUPIXENT. Avoid use of live vaccines during treatment with DUPIXENT.
ADVERSE REACTIONS:
Most common adverse reactions are:
- Atopic Dermatitis (incidence ≥1%): injection site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes simplex virus infection, dry eye, and eosinophilia. The safety profile in pediatric patients through Week 16 was similar to that of adults with AD. In an open-label extension study, the long-term safety profile of DUPIXENT ± TCS in pediatric patients observed through Week 52 was consistent with that seen in adults with AD, with hand-foot-and-mouth disease and skin papilloma (incidence ≥2%) reported in patients 6 months to 5 years of age. These cases did not lead to study drug discontinuation.
- Asthma (incidence ≥1%): injection site reactions, oropharyngeal pain, and eosinophilia.
- Chronic Rhinosinusitis with Nasal Polyps (incidence ≥1% in adult patients): injection site reactions, eosinophilia, insomnia, toothache, gastritis, arthralgia, and conjunctivitis.
- Eosinophilic Esophagitis (incidence ≥2%): injection site reactions, upper respiratory tract infections, arthralgia, and herpes viral infections.
- Prurigo Nodularis (incidence ≥2%): nasopharyngitis, conjunctivitis, herpes infection, dizziness, myalgia, and diarrhea.
- Chronic Obstructive Pulmonary Disease (incidence ≥2%): viral infection, headache, nasopharyngitis, back pain, diarrhea, arthralgia, urinary tract infection, local administration reactions, rhinitis, eosinophilia, toothache, and gastritis.
- Chronic Spontaneous Urticaria (incidence ≥2%): injection site reactions.
- Bullous Pemphigoid (incidence ≥2%): arthralgia, conjunctivitis, vision blurred, herpes viral infections, keratitis.
USE IN SPECIFIC POPULATIONS
- Pregnancy: A pregnancy exposure registry monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy. To enroll or obtain information call 1‑877‑311‑8972 or go to https://mothertobaby.org/ongoing-study/dupixent/. Available data from case reports and case series with DUPIXENT use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier; therefore, DUPIXENT may be transmitted from the mother to the developing fetus.
- Lactation: There are no data on the presence of DUPIXENT in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for DUPIXENT and any potential adverse effects on the breastfed child from DUPIXENT or from the underlying maternal condition.
Please see accompanying full Prescribing Information.
INDICATIONS
Atopic Dermatitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 6 months and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. DUPIXENT can be used with or without topical corticosteroids.
Asthma: DUPIXENT is indicated as an add-on maintenance treatment of adult and pediatric patients aged 6 years and older with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm or status asthmaticus.
Chronic Rhinosinusitis with Nasal Polyps: DUPIXENT is indicated as an add-on maintenance treatment in adult and pediatric patients aged 12 years and older with inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP).
Eosinophilic Esophagitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 1 year and older, weighing at least 15 kg, with eosinophilic esophagitis (EoE).
Prurigo Nodularis: DUPIXENT is indicated for the treatment of adult patients with prurigo nodularis (PN).
Chronic Obstructive Pulmonary Disease: DUPIXENT is indicated as an add-on maintenance treatment of adult patients with inadequately controlled chronic obstructive pulmonary disease (COPD) and an eosinophilic phenotype. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm.
Chronic Spontaneous Urticaria: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 12 years and older with chronic spontaneous urticaria (CSU) who remain symptomatic despite H1 antihistamine treatment. Limitations of Use: DUPIXENT is not indicated for treatment of other forms of urticaria.
Bullous Pemphigoid: DUPIXENT is indicated for the treatment of adult patients with bullous pemphigoid (BP).
CONTRAINDICATION: DUPIXENT is contraindicated in patients with known hypersensitivity to dupilumab or any of its excipients.
WARNINGS AND PRECAUTIONS
Hypersensitivity: Hypersensitivity reactions, including anaphylaxis, acute generalized exanthematous pustulosis (AGEP), serum sickness or serum sickness-like reactions, angioedema, generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. A case of AGEP was reported in an adult subject who participated in the bullous pemphigoid development program. If a clinically significant hypersensitivity reaction occurs, institute appropriate therapy and discontinue DUPIXENT.
Conjunctivitis and Keratitis: Conjunctivitis and keratitis occurred more frequently in AD, COPD, and BP subjects who received DUPIXENT versus placebo, with conjunctivitis being the most frequently reported eye disorder in AD. Conjunctivitis also occurred more frequently in adult CRSwNP and PN subjects who received DUPIXENT compared to those who received placebo. Conjunctivitis and keratitis have been reported with DUPIXENT in postmarketing settings, predominantly in AD patients. Some patients reported visual disturbances (e.g., blurred vision) associated with conjunctivitis or keratitis. Advise patients or their caregivers to report new-onset or worsening eye symptoms. Consider ophthalmological examination for patients who develop conjunctivitis that does not resolve following standard treatment or signs and symptoms suggestive of keratitis, as appropriate.
Eosinophilic Conditions: Patients being treated for asthma may present with clinical features of eosinophilic pneumonia or eosinophilic granulomatosis with polyangiitis (EGPA). These events may be associated with the reduction of oral corticosteroid therapy. Healthcare providers should be alert to vasculitic rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and/or neuropathy presenting in their patients with eosinophilia. Cases of eosinophilic pneumonia were reported in adults who participated in the asthma development program and cases of EGPA have been reported with DUPIXENT in adults who participated in the asthma development program as well as in adults with co-morbid asthma in the CRSwNP development program. Advise patients to report signs of eosinophilic pneumonia and EGPA. Consider withholding DUPIXENT if eosinophilic pneumonia or EGPA are suspected.
Acute Symptoms of Asthma or Chronic Obstructive Pulmonary Disease or Acute Deteriorating Disease: Do not use DUPIXENT to treat acute symptoms or acute exacerbations of asthma or COPD, acute bronchospasm, or status asthmaticus. Patients should seek medical advice if their asthma or COPD remains uncontrolled or worsens after initiation of DUPIXENT.
Risk Associated with Abrupt Reduction of Corticosteroid Dosage: Do not discontinue systemic, topical, or inhaled corticosteroids abruptly upon initiation of DUPIXENT. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a healthcare provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
Patients with Co-morbid Asthma: Advise patients with co-morbid asthma not to adjust or stop their asthma treatments without consultation with their physicians.
Psoriasis: Cases of new-onset psoriasis have been reported with the use of DUPIXENT for the treatment of atopic dermatitis and asthma, including in patients without a family history of psoriasis. In postmarketing reports, these cases resulted in partial or complete resolution of psoriasis with discontinuation of dupilumab, with or without use of supplemental treatment for psoriasis (topical or systemic). Those who continued dupilumab received supplemental treatment for psoriasis to improve associated symptoms. Advise patients to report new-onset psoriasis symptoms. If symptoms persist or worsen, consider dermatologic evaluation and/or discontinuation of DUPIXENT.
Arthralgia and Psoriatic Arthritis: Arthralgia has been reported with the use of DUPIXENT with some patients reporting gait disturbances or decreased mobility associated with joint symptoms; some cases resulted in hospitalization. Cases of new-onset psoriatic arthritis requiring systemic treatment have been reported with the use of DUPIXENT. Advise patients to report new-onset or worsening joint symptoms. If symptoms persist or worsen, consider rheumatological evaluation and/or discontinuation of DUPIXENT.
Parasitic (Helminth) Infections: It is unknown if DUPIXENT will influence the immune response against helminth infections. Treat patients with pre-existing helminth infections before initiating therapy with DUPIXENT. If patients become infected while receiving treatment with DUPIXENT and do not respond to anti-helminth treatment, discontinue treatment with DUPIXENT until the infection resolves. Helminth infections (5 cases of enterobiasis and 1 case of ascariasis) were reported in pediatric patients 6 to 11 years old in the pediatric asthma development program.
Vaccinations: Consider completing all age-appropriate vaccinations as recommended by current immunization guidelines prior to initiating DUPIXENT. Avoid use of live vaccines during treatment with DUPIXENT.
ADVERSE REACTIONS:
Most common adverse reactions are:
- Atopic Dermatitis (incidence ≥1%): injection site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes simplex virus infection, dry eye, and eosinophilia. The safety profile in pediatric patients through Week 16 was similar to that of adults with AD. In an open-label extension study, the long-term safety profile of DUPIXENT ± TCS in pediatric patients observed through Week 52 was consistent with that seen in adults with AD, with hand-foot-and-mouth disease and skin papilloma (incidence ≥2%) reported in patients 6 months to 5 years of age. These cases did not lead to study drug discontinuation.
- Asthma (incidence ≥1%): injection site reactions, oropharyngeal pain, and eosinophilia.
- Chronic Rhinosinusitis with Nasal Polyps (incidence ≥1% in adult patients): injection site reactions, eosinophilia, insomnia, toothache, gastritis, arthralgia, and conjunctivitis.
- Eosinophilic Esophagitis (incidence ≥2%): injection site reactions, upper respiratory tract infections, arthralgia, and herpes viral infections.
- Prurigo Nodularis (incidence ≥2%): nasopharyngitis, conjunctivitis, herpes infection, dizziness, myalgia, and diarrhea.
- Chronic Obstructive Pulmonary Disease (incidence ≥2%): viral infection, headache, nasopharyngitis, back pain, diarrhea, arthralgia, urinary tract infection, local administration reactions, rhinitis, eosinophilia, toothache, and gastritis.
- Chronic Spontaneous Urticaria (incidence ≥2%): injection site reactions.
- Bullous Pemphigoid (incidence ≥2%): arthralgia, conjunctivitis, vision blurred, herpes viral infections, keratitis.
USE IN SPECIFIC POPULATIONS
- Pregnancy: A pregnancy exposure registry monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy. To enroll or obtain information call 1‑877‑311‑8972 or go to https://mothertobaby.org/ongoing-study/dupixent/. Available data from case reports and case series with DUPIXENT use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier; therefore, DUPIXENT may be transmitted from the mother to the developing fetus.
- Lactation: There are no data on the presence of DUPIXENT in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for DUPIXENT and any potential adverse effects on the breastfed child from DUPIXENT or from the underlying maternal condition.
Please see accompanying full Prescribing Information.
INDICATIONS
Atopic Dermatitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 6 months and older with moderate-to-severe atopic dermatitis (AD) whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable. DUPIXENT can be used with or without topical corticosteroids.
Asthma: DUPIXENT is indicated as an add-on maintenance treatment of adult and pediatric patients aged 6 years and older with moderate-to-severe asthma characterized by an eosinophilic phenotype or with oral corticosteroid dependent asthma. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm or status asthmaticus.
Chronic Rhinosinusitis with Nasal Polyps: DUPIXENT is indicated as an add-on maintenance treatment in adult and pediatric patients aged 12 years and older with inadequately controlled chronic rhinosinusitis with nasal polyps (CRSwNP).
Eosinophilic Esophagitis: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 1 year and older, weighing at least 15 kg, with eosinophilic esophagitis (EoE).
Prurigo Nodularis: DUPIXENT is indicated for the treatment of adult patients with prurigo nodularis (PN).
Chronic Obstructive Pulmonary Disease: DUPIXENT is indicated as an add-on maintenance treatment of adult patients with inadequately controlled chronic obstructive pulmonary disease (COPD) and an eosinophilic phenotype. Limitations of Use: DUPIXENT is not indicated for the relief of acute bronchospasm.
Chronic Spontaneous Urticaria: DUPIXENT is indicated for the treatment of adult and pediatric patients aged 12 years and older with chronic spontaneous urticaria (CSU) who remain symptomatic despite H1 antihistamine treatment. Limitations of Use: DUPIXENT is not indicated for treatment of other forms of urticaria.
Bullous Pemphigoid: DUPIXENT is indicated for the treatment of adult patients with bullous pemphigoid (BP).
CONTRAINDICATION: DUPIXENT is contraindicated in patients with known hypersensitivity to dupilumab or any of its excipients.
WARNINGS AND PRECAUTIONS
Hypersensitivity: Hypersensitivity reactions, including anaphylaxis, acute generalized exanthematous pustulosis (AGEP), serum sickness or serum sickness-like reactions, angioedema, generalized urticaria, rash, erythema nodosum, and erythema multiforme have been reported. A case of AGEP was reported in an adult subject who participated in the bullous pemphigoid development program. If a clinically significant hypersensitivity reaction occurs, institute appropriate therapy and discontinue DUPIXENT.
Conjunctivitis and Keratitis: Conjunctivitis and keratitis occurred more frequently in AD, COPD, and BP subjects who received DUPIXENT versus placebo, with conjunctivitis being the most frequently reported eye disorder in AD. Conjunctivitis also occurred more frequently in adult CRSwNP and PN subjects who received DUPIXENT compared to those who received placebo. Conjunctivitis and keratitis have been reported with DUPIXENT in postmarketing settings, predominantly in AD patients. Some patients reported visual disturbances (e.g., blurred vision) associated with conjunctivitis or keratitis. Advise patients or their caregivers to report new-onset or worsening eye symptoms. Consider ophthalmological examination for patients who develop conjunctivitis that does not resolve following standard treatment or signs and symptoms suggestive of keratitis, as appropriate.
Eosinophilic Conditions: Patients being treated for asthma may present with clinical features of eosinophilic pneumonia or eosinophilic granulomatosis with polyangiitis (EGPA). These events may be associated with the reduction of oral corticosteroid therapy. Healthcare providers should be alert to vasculitic rash, worsening pulmonary symptoms, cardiac complications, kidney injury, and/or neuropathy presenting in their patients with eosinophilia. Cases of eosinophilic pneumonia were reported in adults who participated in the asthma development program and cases of EGPA have been reported with DUPIXENT in adults who participated in the asthma development program as well as in adults with co-morbid asthma in the CRSwNP development program. Advise patients to report signs of eosinophilic pneumonia and EGPA. Consider withholding DUPIXENT if eosinophilic pneumonia or EGPA are suspected.
Acute Symptoms of Asthma or Chronic Obstructive Pulmonary Disease or Acute Deteriorating Disease: Do not use DUPIXENT to treat acute symptoms or acute exacerbations of asthma or COPD, acute bronchospasm, or status asthmaticus. Patients should seek medical advice if their asthma or COPD remains uncontrolled or worsens after initiation of DUPIXENT.
Risk Associated with Abrupt Reduction of Corticosteroid Dosage: Do not discontinue systemic, topical, or inhaled corticosteroids abruptly upon initiation of DUPIXENT. Reductions in corticosteroid dose, if appropriate, should be gradual and performed under the direct supervision of a healthcare provider. Reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
Patients with Co-morbid Asthma: Advise patients with co-morbid asthma not to adjust or stop their asthma treatments without consultation with their physicians.
Psoriasis: Cases of new-onset psoriasis have been reported with the use of DUPIXENT for the treatment of atopic dermatitis and asthma, including in patients without a family history of psoriasis. In postmarketing reports, these cases resulted in partial or complete resolution of psoriasis with discontinuation of dupilumab, with or without use of supplemental treatment for psoriasis (topical or systemic). Those who continued dupilumab received supplemental treatment for psoriasis to improve associated symptoms. Advise patients to report new-onset psoriasis symptoms. If symptoms persist or worsen, consider dermatologic evaluation and/or discontinuation of DUPIXENT.
Arthralgia and Psoriatic Arthritis: Arthralgia has been reported with the use of DUPIXENT with some patients reporting gait disturbances or decreased mobility associated with joint symptoms; some cases resulted in hospitalization. Cases of new-onset psoriatic arthritis requiring systemic treatment have been reported with the use of DUPIXENT. Advise patients to report new-onset or worsening joint symptoms. If symptoms persist or worsen, consider rheumatological evaluation and/or discontinuation of DUPIXENT.
Parasitic (Helminth) Infections: It is unknown if DUPIXENT will influence the immune response against helminth infections. Treat patients with pre-existing helminth infections before initiating therapy with DUPIXENT. If patients become infected while receiving treatment with DUPIXENT and do not respond to anti-helminth treatment, discontinue treatment with DUPIXENT until the infection resolves. Helminth infections (5 cases of enterobiasis and 1 case of ascariasis) were reported in pediatric patients 6 to 11 years old in the pediatric asthma development program.
Vaccinations: Consider completing all age-appropriate vaccinations as recommended by current immunization guidelines prior to initiating DUPIXENT. Avoid use of live vaccines during treatment with DUPIXENT.
ADVERSE REACTIONS:
Most common adverse reactions are:
- Atopic Dermatitis (incidence ≥1%): injection site reactions, conjunctivitis, blepharitis, oral herpes, keratitis, eye pruritus, other herpes simplex virus infection, dry eye, and eosinophilia. The safety profile in pediatric patients through Week 16 was similar to that of adults with AD. In an open-label extension study, the long-term safety profile of DUPIXENT ± TCS in pediatric patients observed through Week 52 was consistent with that seen in adults with AD, with hand-foot-and-mouth disease and skin papilloma (incidence ≥2%) reported in patients 6 months to 5 years of age. These cases did not lead to study drug discontinuation.
- Asthma (incidence ≥1%): injection site reactions, oropharyngeal pain, and eosinophilia.
- Chronic Rhinosinusitis with Nasal Polyps (incidence ≥1% in adult patients): injection site reactions, eosinophilia, insomnia, toothache, gastritis, arthralgia, and conjunctivitis.
- Eosinophilic Esophagitis (incidence ≥2%): injection site reactions, upper respiratory tract infections, arthralgia, and herpes viral infections.
- Prurigo Nodularis (incidence ≥2%): nasopharyngitis, conjunctivitis, herpes infection, dizziness, myalgia, and diarrhea.
- Chronic Obstructive Pulmonary Disease (incidence ≥2%): viral infection, headache, nasopharyngitis, back pain, diarrhea, arthralgia, urinary tract infection, local administration reactions, rhinitis, eosinophilia, toothache, and gastritis.
- Chronic Spontaneous Urticaria (incidence ≥2%): injection site reactions.
- Bullous Pemphigoid (incidence ≥2%): arthralgia, conjunctivitis, vision blurred, herpes viral infections, keratitis.
USE IN SPECIFIC POPULATIONS
- Pregnancy: A pregnancy exposure registry monitors pregnancy outcomes in women exposed to DUPIXENT during pregnancy. To enroll or obtain information call 1‑877‑311‑8972 or go to https://mothertobaby.org/ongoing-study/dupixent/. Available data from case reports and case series with DUPIXENT use in pregnant women have not identified a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. Human IgG antibodies are known to cross the placental barrier; therefore, DUPIXENT may be transmitted from the mother to the developing fetus.
- Lactation: There are no data on the presence of DUPIXENT in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for DUPIXENT and any potential adverse effects on the breastfed child from DUPIXENT or from the underlying maternal condition.
Please see accompanying full Prescribing Information.
This site is intended for US payers, formulary committees, or other similar entities for purposes of population-based drug selection, coverage, and/or reimbursement decision-making, pursuant to FD&C Act Section 502(a).
© 2025 Sanofi and Regeneron Pharmaceuticals, Inc. All Rights Reserved.
DUPIXENT® and DUPIXENT MyWay® are registered trademarks of Sanofi Biotechnology.
Sanofi US is hosting this website on behalf of Sanofi and Regeneron Pharmaceuticals, Inc. Sanofi and Regeneron are industry partners, who are committed to handling personal data in ways that respect your privacy. Both companies may independently process your personal data to manage patient support programs and product marketing campaigns. Please refer to Regeneron’s Privacy Notice and Sanofi’s Privacy Policy and Cookies Policy for more information regarding processing of your personal data.
BOREAS and NOTUS clinical study designs1,a
Two Phase 3 trials evaluated the efficacy of DUPIXENT + standard of careb administered every 2 weeks in patients with inadequately controlled COPD.1,b
Standard of care was triple inhaled therapy (LAMA + LABA + ICS.2
Patients with a history of asthma were excluded from the BOREAS and NOTUS trials.
a1874 patients were enrolled in the BOREAS (N=939) and NOTUS (N=935) trials.1
b98% received LAMA + LABA + ICS in BOREAS and 99% in NOTUS.1
COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; Q2W, once every 2 weeks; SC, subcutaneous.
Study designs: endpoints1
| PRIMARY ENDPOINT | Week 52 | Annualized rate of moderate or severe COPD exacerbations |
|---|---|---|
| SELECT SECONDARY ENDPOINTS | Week 12
Week 52 |
Change in lung function (pre-bronchodilator FEV₁) from baseline |
| Week 52 | Change in SGRQ total score from baseline | |
| Week 52 | Percentage of patients with SGRQ total score improvement of ≥4 points |
FEV1, forced expiratory volume in 1 second; SGRQ, St. George’s Respiratory Questionnaire.
Study designs: inclusion and exclusion criteria3,4
aModerate exacerbations were defined as exacerbations that resulted in treatment with a systemic glucocorticoid, an antibiotic agent, or both. Severe exacerbations were defined as exacerbations that led to hospitalization or an emergency medical care visit or that resulted in death.1
DUPIXENT improved SGRQ total score at Week 521
DUPIXENT reduced SGRQ scores—lower SGRQ scores indicate improved quality of life.1,3,4
BOREAS trial 3
BOREAS trial 3
In NOTUS, patients receiving DUPIXENT + standard of care (n=362) experienced -9.8 reduction in total SGRQ score vs -6.4 in patients with placebo + standard of care (n=359) (LSM difference: -3.4 [95% CI: -5.8, -0.9])
NOTUS results are descriptive. Definitive conclusions cannot be made.
Standard of care was triple inhaled therapy (LAMA + LABA + ICS.2
ICS, inhaled corticosteroid; LABA, long-acting beta agonist; LAMA, long-acting muscarinic antagonist; LSM, least squares mean; SGRQ, St. George’s Respiratory Questionnaire